Recurrent Herpes Zoster Keratitis
Purpose. Herpetic eye disease, which includes both herpes zoster and herpes simplex, can lead to severe eye complications. Managing recurrent cases can be particularly challenging. Herpetic Eye Disease Study (HEDS I and II) has provided evidence-based strategies for handling herpes simplex infections and their recurrences. More recently, the Zoster Eye Disease Study (ZEDS) has focused on offering evidence-based treatments specifically for herpes zoster infections and recurrences. This article aims to highlight a case of recurrent zoster-related keratitis and discusses the diagnosis and appropriate treatment options.
Material and Methods. An 87-year-old Caucasian patient with a history of previous Herpes Zoster Ophthalmicus (HZO) related keratitis presented with a new corneal epithelial defect. His clinical diagnosis was a recurrent herpes zoster-related keratitis. The patient was properly educated on the diagnosis and treatment.
Results. The herpetic zoster keratitis was successfully treated with long-term oral valacyclovir, antibiotic coverage, and additional topical lubrication.
Conclusion. This case discusses the diagnosis and management of recurrent herpes zoster keratitis. Due to the recurrent nature of herpetic eye disease, it is crucial to be aware of the need for ongoing prophylactic antiviral treatment and the importance of regular clinical surveillance.
Introduction
Herpes simplex and herpes zoster viruses are large, double-stranded DNA viruses that can lead to serious eye infections and recurrent disease.1 The ocular manifestations of herpetic eye diseases can impact both the anterior and posterior segments of the eye and can have devastating visual consequences. Scarring from herpetic keratitis is a major cause of infectious blindness worldwide.2
Primary herpes simplex ophthalmicus infections are transmitted through oral and facial mucous membranes or via the birth canal, and most commonly present as blepharconjunctivitis. Once the initial infection has resolved, the virus remains latent in the trigeminal ganglion and can reactivate later in life, most commonly affecting the anterior segment of the eye.1
Herpes Zoster is a result of the reactivation of the varicella zoster virus, the same virus responsible for chickenpox.3 Approximately 98 % of people aged 40 and older worldwide have had chickenpox at some point in their lives. The initial varicella infection spreads through respiratory droplets and direct contact with fluid emanating from the blisters.4 Only individuals who have previously been infected with the varicella virus—either through natural infection or vaccination—can develop herpes zoster. After the initial infection is resolved, the virus remains dormant in the dorsal root ganglia. When the varicella virus reactivates later in life, it typically presents as a painful rash.5
The risk of developing herpes zoster increases significantly after the age of 50, as well as in individuals with weakened immune systems.6 Every year, millions of new cases are diagnosed globally.7
Case presentation
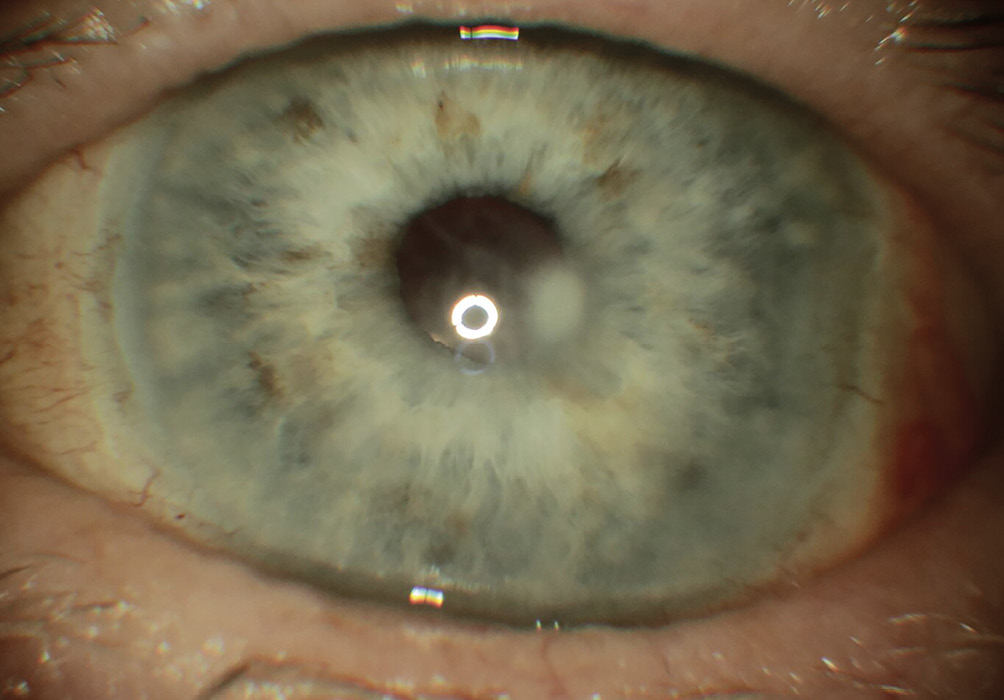
An 87-year-old Caucasian male presents with eye pain and decreased vision in the left eye (OS) for the past two days. He denies any discharge or trauma. His ocular history includes cataract extraction in both eyes (OU) two years ago and a history of Herpes Zoster Ophthalmicus (HZO) one year ago, which was complicated by corneal keratitis that was treated by an outside provider. His medical history is notable for well-controlled diabetes mellitus (Hemoglobin A1c: 5.9 % / 41 mmol/mol), hypertension managed with valsartan and hydrochlorothiazide, and hyperlipidemia controlled with atorvastatin.
Upon examination, his best corrected visual acuity was 20/40 in the right eye (OD) and 20/150 in the left eye (OS), with no improvement on Pinhole testing. Pupils and ocular motility were within normal limits. Slit lamp examination in the right eye was unremarkable, while the left eye demonstrated diffuse grade 2+ injection and a central corneal epithelial defect measuring 1.5 mm in diameter, with underlying stromal haze and no edema. The anterior chambers were deep and quiet in both eyes. Corneal sensitivity testing using a cotton tip applicator indicated reduced sensitivity OS compared to OD. Intraocular pressures were measured at 10 mmHg in both eyes using Goldmann tonometry.
A dilated fundus exam was unremarkable.
The patient was diagnosed with recurrent HZO keratitis OS with epithelial ulceration. He was started on 1000 mg of valacyclovir orally three times daily for seven days (his most recent BUN (Blood Urea Nitrogen) and creatinine levels were within acceptable ranges), along with erythromycin ointment at night for prophylaxis against secondary bacterial infection. He was scheduled for a follow-up visit in 24 hours. At the 24-hour follow-up, the clinical findings remained unchanged. At the 72-hour follow-up, the epithelial corneal defect had diminished to 0.5 mm, and by one week, the epithelial defect had resolved, with the stromal scar remaining. Visual acuity improved to 20/80 in OS. A topical steroid, prednisolone acetate 1 %, was introduced four times daily. Records obtained from the patient’s previous doctor indicated residual stromal scarring following the initial HZO keratitis infection, with a best-corrected visual acuity of 20/80. Topical moxifloxacin and erythromycin were discontinued. Given that the stromal scar was longstanding, it was decided to taper the topical steroid. The patient continued on valacyclovir 1000 mg daily, preservative-free artificial tears four to six times a day, and a lubricating ointment at night. He was monitored with follow-up visits every two months, eventually transitioning to monthly visits with no recurrences. His BUN and creatinine levels are checked every three months.
Discussion
Herpes zoster is often referred to as „Shingles“. It is primarily characterized by painful vesicular dermatitis that is localized to a specific dermatome supplied by a spinal or cranial sensory ganglion. The vesicular rash is typically unilateral and stops abruptly at the midline of the involved dermatome‘s sensory coverage.8 Initiating oral antiviral therapy within 72 hours of rash onset is crucial for reducing the duration and severity of the disease.9
The post-herpetic neuralgia (PHN) phase is characterized by persistent pain that lasts for 30 days or more after all lesions have crusted. Symptoms can vary from mild, short-term itchiness to debilitating pain that may be severe and incapacitating. Patients report various types of pain, including burning, shooting, sharp, throbbing, and tender sensations. The discomfort is usually confined to the original dermatome and can persist for weeks, months, or even years.10
The mean age of onset of HZV is 52, and the World Health Organization recommends that countries consider vaccinating healthy adults 50 and over using the recombinant herpes zoster vaccine. Shingrix contains an inactivated form of the varicella-zoster virus ( recombinant vaccine) and provides strong protection against shingles & post-herpetic neuralgia.11
Potential systemic complications associated with herpes zoster include aseptic meningitis, encephalitis, vasculitis, myelitis, bacterial superinfection, Bell’s Palsy, and Ramsay Hunt Syndrome. Zoster and postherpetic neuralgia (PHN) significantly increase the risk of depression, anxiety, and suicidal thoughts. Research has shown that within 90 days of the onset of zoster, 55 % of patients experience symptoms of depression and anxiety. By 180 days after the rash appears, 45 % of patients continue to suffer from depression due to PHN.12 There is also a 1.9 times increased risk of stroke within 30 days of the infection.13 Studies have shown that herpes zoster may increase the risk of developing dementia, potentially due to factors such as neuroinflammation or cerebral vasculopathy. Additionally, research indicates that the recombinant zoster vaccine can result in a decreased risk of dementia, reflecting an additional benefit of vaccination.14 A specific study conducted at Stanford found that the vaccine cuts the risk of dementia by 20 %.15,16
Herpes Zoster Ophthalmicus (HZO) accounts for up to 25 % of all herpes zoster cases. It affects the dermatome of the trigeminal nerve, specifically the ophthalmic division (V1). The trigeminal nerve (cranial nerve V) is divided into three main branches: V1 (ophthalmic), V2 (maxillary), and V3 (mandibular). Infection and inflammation related to herpes zoster can affect any adnexal, ocular, or orbital structure. Complications may include eyelid scarring, notching, loss of cilia, trichiasis, cicatricial entropion, and various ocular issues such as episcleritis or scleritis. More severe complications can involve keratitis, uveitis, trabeculitis, pupil anomalies, glaucoma, occlusive arteritis, acute retinal necrosis, and cranial nerve palsies, as well as optic neuropathy.2
A treatment protocol for herpes zoster eye disease has been developed by the New York University-sponsored Herpes Zoster Eye Disease Study (ZEDS), conducted from August 2017 to June 2024.17
The primary study aimed to assess whether a 12-month course of suppressive antiviral therapy with 1000 mg daily oral valacyclovir decreased the rate of new or worsening ocular manifestations of HZO. These included dendritic epithelial keratitis, stromal keratitis, endothelial keratitis, and iritis. The secondary objective was to evaluate whether there is a lasting benefit from the treatment at the 18-month mark, which is six months after treatment cessation. This also included determining whether a 12-month treatment with 1000 mg daily of oral valacyclovir decreased the severity and duration of postherpetic neuralgia at both the 12-month and 18-month follow-ups. Key findings indicate that evidence supports the use of 1000 mg of valacyclovir daily to reduce the occurrence of new or worsening ocular manifestations related to herpes zoster. It also significantly lowered post-herpetic neuralgia pain scores at 12 and 18 months.18
Conclusion
Herpes Zoster Ophthalmicus, whether presenting initially or as a recurrent condition, has the potential to cause significant and lasting ocular complications. Early diagnosis, along with prompt treatment, is crucial for improving patient outcomes. Notably, findings from the ZEDS study suggest that individuals experiencing recurrent herpes zoster infections may greatly benefit from prolonged use of antiviral medications. This can help mitigate the frequency and severity of herpes zoster, preserving vision and overall eye health.
Conflicts of Interests
The authors declare that there is no conflict of interests regarding the methods and devices mentioned in the article.